Historical trivia - the Circulation and the Cardiac cycle.
- May 7, 2022
- 16 min read
Updated: Feb 9
Hippocrates of Kos (460 B.C.- 370 B.C.), a Greek philosopher and physician of the classical period, is considered the Father of Medicine. The Hippocratic oath is still followed today. Observation, reasoning, and occasional cadaveric dissection were the only tools the early clinicians had for diagnostic purposes. Even the great Galen had little exposure to human dissection and surmised or extrapolated from the dissection of macaque monkeys. In or before the Hippocratic times, the Greeks were considered the most knowledgeable in medical matters. The Greeks, including Hippocrates till Galen, believed that circulation was made up of two systems – arterial and venous. The Greko-Romans also had an astounding idea that sputum and pleural effusions were formed by the brain, and Galen forwarded a theory that venous blood was created in the liver and the venous blood crossed over across multiple invisible holes in the interventricular septum in the heart. Numerous peripheral unexplained anastomoses were also involved. Pneuma or air entered the blood via the lung veins, and the invisible holes in the septum of the heart allowed admixture. The arteries contained both air and blood, and arterial blood was a mixture of air and blood.
Intestinal digestion and the production of nutrients that were carried to the cells by blood were accepted by all. Even before Galen, there were ancient notions as summarised ---
1. The four elements of nature are the earth, wind, fire, and water.
2. These were embodiments of the four primary irreducible qualities, such as hot, cold, dry, and wet.
3. These represented the corresponding humours of the body, like the blood, black bile, yellow bile, and phlegm.
4. The humours were food-derived.
Diseases represented an imbalance of the humors, and treatment was directed at the restoration of this balance. There was an intimate relationship with blood that was being circulated. It was believed that the assimilated and absorbed intestinal food was converted into blood in the liver. Galen believed that yellow and black bile mixed with blood and were distributed throughout the body. Only a portion of blood (‘natural spirits’) entered the heart. The pneuma or air (‘vital spirits’) enters the blood in the lungs. In the left ventricle of the heart, which is reached via the invisible pores in the interventricular septum, the blood is mixed with ‘vital spirits’, and this arterial blood thus formed, is distributed to the tissues. The humors, spirits, and heat flowed within the organs according to need and were the main reason behind living qualities. A small portion of arterial blood also goes to the brain, and is further refined to help the psychic spirits work.
The Greeks and the Egyptians recorded the early historical accounts of heart dissection. They forwarded an idea intermingled with that of the religious beliefs, magic, and mystical facts. The Egyptians learned from mummification processes and animal dissection due to a religious and cultural ban on cadaveric dissections and understood that, as the heart was more or less centrally positioned, it had some essential functions. The heart was considered the seat of the soul and a recorder of the deeds of life. It was measured against feathers, and the lighter the heart, the purer the soul of the departed individual. In the living, the Egyptians held the heart in high esteem and considered the heart to be the central organ of thought, emotion, soul, and production of bodily fluids. They also knew that vessels were distributed to the peripheral parts, but they confused them with similar tubular structures and considered these to transport many bodily fluids mixed with pneuma and vital spirits. Egyptians held the centre stage in medical practice from the 19th to the 16th century B.C. The Egyptian medical papyri, such as the Edwin Smith papyrus, the George Eber papyrus, the German Heinrich Brugsch papyrus, etc., are all evidence of how a patient was cared for at that time and the prevailing thoughts and practices. For the next thousand years, no new document was found. By the 6th century, we find that temples in Egypt were reconstructed and an adjacent attached “House of Healing” constructed. The priests were secretly taught healing techniques, and there are no records of how.
There was a lot of intermingling across the Mediterranean, especially between the Egyptians and the Greeks, and it was natural that the latter dominated the scene next.
The ancient Greeks were thinkers and furthered the Egyptian beliefs. Before the Hippocratic corpus, other stalwarts pondered circulation. In the Hippocratic corpus, there is a compilation called “On the Heart” that details the topographic anatomy and also mentions the presence of two ventricles as chambers of the heart. There was the mention of veins being distributed throughout the body in other treatises of the Hippocratic corpus, the collections 'On Nutriment' and ‘On Joints'. But these veins originated from the umbilicus, and the purpose of their connection with the heart was not explained. Asclepios was considered the first person to possess significant knowledge about the cardiovascular system before Hippocrates organized, systematized, and showed the path to scientific thinking in medicine. After him came the names of Alcmaen, Empedocles, Diogenes of Apollonia, etc. In the 4th century, the most notable Greek after Hippocrates was Synnesis, of Syria. There was a fierce debate among philosophers about the role of the heart and the brain, and it was accepted that while the heart was the soul, vascular supply to the brain regulated sleep and associated disorders.
The Greeks also had by this time advanced the name “cardia” for the heart, recognized the two ventricles, discarded Plato's theory that the heart is a knot of veins, and there were two auricles or ear-shaped venous dilatations as the veins approached the heart.
Aristotle’s appearance in the 3rd century B.C. showed a different scene, and he was responsible for forwarding the cardio-centric theory. Though he documented extensive dissections in detail, there were some glaring mistakes. He maintained that there were three ventricles, and he was not sure of the position of the heart. He dissected the pulmonary system of vessels also.
The considered golden age for ancient Greek medicine was around the 4th century. The earliest references we have are those of Praxagorus, Aristotle, Herophilus, and Erasistratus. It was ironic that even during these early times, Aristotle (340 B.C.) believed that the heart was the centre of all physiological mechanisms and the soul. Blood vessels originated here. Praxagorus, around the same time, was also able to differentiate between arteries and veins. Herophilus showed that arteries had a thicker wall. The lung happened to be a notable exception. Though Erasistratus believed that both arteries and veins originated in the heart, he also had the flawed belief of the time that the arteries were full of pneuma or air. To explain blood coming out of arteries following an accidental prick, the ancient Greeks used to say that it was venous blood moving into arteries via invisible anastomoses. The 'heart' of the body was an innate property and linked intimately to soul and spirit, and nature had a hand in it.
Aristotle is considered the first person to recognize the heart as the central and most important organ of an individual. However, he could not alienate himself from the mystical ideas that surrounded the organ taught at that time. He was accurate as he was bold enough to state that the heart was “the source of all movement since the heart links the soul with the organs of life”. The rhythmical and constant beat of the heart from birth to death was well-known from the very beginning. That the upstroke of the pulse coincides with the contraction of the heart was also well known. Though early Egyptians are credited, this fact was universal, and some clinical practices even emphasized the importance of the pulse examination. The Ayurvedic practice had ‘vayu’, ‘pitta’, and ‘kaph’ as equivalents of the four humours in Western medicine. The pulse was also known as the ’nari’ with a deeper accent to the ‘r’ and the tip of the three fingers was used to examine the pulse. A thorough examination of the pulse and understanding of the physical and mental state of a person, together with the ability to predict the course of the disease, was considered supreme.
The Greeks introduced the term ‘cardia' for the heart and also called the earlike projections, the ‘auricles’, after veins joined the heart. Leonardo da Vinci first recognized that the human heart was four-chambered. The thick-walled ventricles were the actual pumping chambers.
With Harvey’s revolutionary theory of the method of circulation, the horizon opened for the development of techniques for visualization of the beating organ.
Cardiothoracic and vascular surgery has a varied history. Vascular surgery is said to have developed definitively after the pioneering works of Carel & Guthrie. Operations on other thoracic organs were explored once endotracheal intubation was established and the effect of higher atmospheric pressure on the lower intra-thoracic pressure could be tackled easily. Initially cardiac surgery was not considered possible as –
Surgery on a constantly moving organ was not deemed feasible,
There was the constant risk of fatal arrhythmias,
Visibility of joinable tissue margins were not considered possible in the presence of unabated bleeding,
Tissue union and healing were doubted.
Not knowing the technique of stopping the heart in a relaxed suturable state and maintenance of brain circulation and tissue oxygenation during a hypothetical period of circulatory bypass of the heart and lung,
Method or medicine not known for preventing intravascular clot formation and keeping the blood in a fluid state within the circulatory network.
In 1896, Rehn created a feat which was considered a landmark. He was made to repair a right
ventricular stab wound with two interrupted horsehair sutures mounted on the smallest and thinnest needle available at that time. This was the beginning of cardiac surgery. Discovery and use of heparin, DeBakey’s promotion of Porter-Bradley pump as the Heart-Lung machine, Gibbon’s successful use of the heart-lung machine for repair of an intracardiac defect, and gradual evolution of the oxygenators were, among other factors, responsible for the improved state of cardiac surgery today.
Galen was trained with these convoluted beliefs and mystical ideas of soul and spirits. He believed in them. Fitting in the right organ and attributing to it the proper physiological function was difficult at that time. He had good reasoning qualities and tried his best to conform to the vicaries of nature during his life demonstrations. He had his own beliefs and theorized that veins were the main carriers of blood, and they originated in the liver of the organism. He believed that the heart intrinsically pulsates and the lungs during respiration cool the innate heat and produce vital spirits. Pulsation of the arteries was an intrinsic property and the whole-body breaths. No part of the body was pure, and each part had something of a part of pneuma, soul, and vital spirit.
Galen was short on human dissection experience as there was a ban on such procedures. Though the school in Alexandria had permission and Galen was trained there, his experience was not adequate. He could get access only during a gladiatorial death and dissection of Barbary monkeys. He mostly depended upon extrapolation from such dissections, reasoning, and imagination. Being the Emperor's physician, he was respected and believed by all.
Early treatment was based on an effort to restore balance. Bloodletting and application with tightening were mainstays in treatment procedures with the intent of diverting blood from the affected parts. Medicines were available substances that had observational relief of symptoms and agents hypothesized to have beneficial values.
Galen’s doctrines were followed for centuries. After the fall of the Roman Empire, the Church became powerful, and the religious beliefs of that period reconciled well with Galen’s views. This continued from 500 to 14000 A.D., covering the dark and Middle Ages. Though historically dissection was started in Salerno in the 12th century, human body dissection took off at the University of Bologna in Italy, for the next 3 centuries. Every attempt was made at fitting the findings to Galen’s teachings.
This four humors theory became a prevalent medical theory for over a millennium. The theory experienced widespread popularity throughout the Middle Ages with useful additions from Aristotle, Galen, Paracelsus, Adicke, and others, in different centuries. and the term “humorism” (also humoralism) was used. These ‘humors’ were seasonal and the table that follows summarises the popular belief of the middle ages and the approximate timelines –
TIMELIINE | NAME | HUMOURS | |||
Middle ages - Rediscovery & revision 18th century- Popularisation 20th century - Modernization & inclusion in curriculum | Hippocrates (Greek) | Blood | Yellow bile | Black bile | Mucous |
325 B.C. Sources of happiness | Aristotle (Greek) | Hedone (sensuous pleasure) | Ethicos (moral virtue) | Proprietary (acquiring assets) | Calm or unemotional |
A.D. 190 Temperaments & organ of origin | Galen (Greek) | Sanguine liver | Choleric gall-bladder | Melancholic spleen | Phlegmatic lungs |
A.D. 1550 Proposed totem spirits | Paracelsus (Swiss alchemist) | Curious sylph (a mythical, ethereal spirit of the air) | Changeable salamander (a lizard-like amphibian with immense regrowth potential & colour-changing ability in some varieties) | Industrious gnome (a mythological, subterranean earth spirit guarding treasure, often depicted as a small, bearded humanoid) | Inspired undines (mermaid or water spirit) |
During Hippocrates’ period, i.e. 400 B.C., people believed that there was a causal relationship between -
Symptomatic expression of disease,
Environmental elements,
Organ of origin,
The four seasons, and
Mental character.
The four Hippocratic humours were suggested around this period, and the diagnosis & treatment of a disease consisted of a mix & match of the appropriate humour with the factors described above. Circumstantial evidence, superstitions, attitude and feeling of the physician, and the method/s adopted for management all had a bearing on the overall treatment of the patient. Aristotle, around 325 B.C., after Hippocrates, put forward systematic observation, logic, and dissection to understand mammalian biology and health. He was instrumental in guiding medical practice away from social superstitions , emphasizing empirical evidence, laying the philosophical and methodological basis for scientific inquiry in medicine. Thus he came to be known as the “godfather of evidence based medicine”. Clinical methods were organised and logical step-wise elicitation could be possible after the discovery and introduction of percussion by Auenbrugger, its subsequent popularisation by Corvisart, and the invention and establishment of the stethoscope for enhanced auscultation of body sounds by Laenec.
The oriental practice was concerned with other things and was less interested in heart & circulation. The Arabs & Byzantines had better access to ancient Grecian medical practice and many writings were translated with their input. It was found that the Arab ibn Al-Nafis of Damascus gave the first description of lung circulation in the 13th century. The mere description of circulation to the lung is mired in controversy. Some say that it was Hippocrates who described a lung-based lesser circulation, but its intimate relationship with the main circulatory system remains unexplained. They were so engrossed with soul, pneuma, vital spirits, and other mystical things, that a simplified explanation eluded them.
The Muslims and the Arabs had better access to Greek compilations of that time. Even Avicenna, as he is known to the Westerners, integrated the early Greek teachings with those of Galen and mentioned mystical features in his book The Canon of Medicine. It is recorded that Ibn Al-Nafis of Damascus in the 13th century described pulmonary circulation in detail. Another Syrian, Qusta Ibn Luca, drew several figures and tried to show that his fellow countryman was right. The findings of the Spanish physician Michael Servatus, in the 14th century, and the Italian clinician Realdo Colombo at about the same time were incidental independent events. These were difficult times, and the general population was steeped in religious beliefs. Whoever was a non-believer of the ideas of the Church's ideas was burned at the stake. Michel Servatus, along with his books, suffered the same fate.
Vesalius was responsible for disproving the Galenian belief of invisible pores in the interventricular septum with his dissections on human cadavers. The Renaissance occurred during the 14th century and ushered in new ideas and thoughts. It was not until the reign of Charles I and the early 15th century did William Harvey put forward his seminal work on circulation. He was the Lumleian lecturer at King's College at that time, and not only was his work path-breaking, but he also defended it and immortalized it in his book ‘De Motu Cordis et Sanguinis in Animalibus (1628)'. That circulation was continuous, and a single system perfusing the whole body was monumental. All his life, he had to defend the idea that the heart acted as a pump and arterial blood is distributed evenly to the periphery and gets cooled before being returned by the one-way valved venous system. He summarised his findings in the 13th chapter of the book and was able to convince others that pulmonary circulation was, in fact, an integral part of the circulatory loop. He was at first not believed by his peers, and then he had critics whom he answered by performing and documenting experiments. The later book 'Exercitationes Duae Anatomical de Sanguinis, ad Joannem Riolanem, Filum, Parisiensem’ details the response.
It was astonishing to see men blindly following the doctrines of Galen for such a long time. Only some accurate drawings were seen by the great Leonardo da Vinci during the Renaissance period, and the dynamics of blood flow were learned. He had his fingers in too many pies, and the next notable discovery was of capillaries that connected the arterial and venous systems at the tissue level. Marcelo Malpighi was armed with a microscope and was able to visualize Harvey’s assumptions (1661).
Little happened thereafter, and the anatomists recorded their findings as they observed. Leonardo da Vinci was one such keen observer and drew what he saw during dissection. However, Leonardo noticed that “all the veins and arteries arise from the heart. The reason for this is that the maximum thickness found in the veins and arteries occurs at the junction where they meet the heart. The more removed they are from the heart, the thinner they become and divide into smaller branches.”
Harvey’s work is still considered one of the greatest discoveries, and he was the first to show a relationship between the heart and the blood that was flowing in the vessels connecting with it. Also, his work enabled physicians to discard mystical ideas about ‘pneuma’ and ‘spirit’. However rare it may be, he was instrumental in showing the possibility of air or gas embolism when introduced into the bloodstream. Harvey was a friend of King Charles I and was allowed to dissect carcasses and observe during the king’s deer hunts. Unifying and schematically linking circulation with the heart was not so easy, but his conviction ultimately made a mark. Further knowledge was acquired by observation and dissection thereafter, and the events were experimentally proven and documented.
So now we know that the heart has two ventricles and two atria, i.e., four (4) chambers. The atria are the receiving chambers, and the ventricles eject blood by muscular contraction to act as a pump and distribute blood throughout the circulatory system. The atrioventricular valves are at the entry of the ventricles, and “sigmoid” or semilunar valves prevent backflow into the ventricles. The pulmonary system differs structurally due to the low pressures in the system, and this is a circulatory scheme where venous blood is in the arteries and oxygenated bright red blood is in the veins. Systole is the term for contraction of the heart, and diastole is the period of relaxation. There is an inherent conduction pathway with self-rhythmic signal generation, allowing the heart to beat throughout life. Normally, atrial contraction precedes ventricular contraction by milliseconds. Otherwise, contraction of the heart is a synchronous process enabling continuous circulation. The usual time taken for a period of a single relaxation and a single contraction is 0.8 seconds. Several events occur in a sequence during the cardiac cycle. In addition to clinical methods, several investigations and tests have evolved to diagnose heart ailments and to see the pathophysiology that may offer prognostic insights. Most of them can be represented graphically. Carl Wiggers, in 1906, was able to combine all the graphical parameters in one diagram in conjunction with the events in the cardiac cycle. This was an attempt basically at describing the normal physiological events and helping in teaching. Around the same period, Willem Einthoven developed doctors’ ability to depict the heart and its parts, functions, and illnesses, depicting the magnified view of the inherent electrical activity of the heart. The venous pulse waveforms and simultaneous recording of carotid pulse with a photo-plethysmograph and recording of heart sound with time-event plotting on paper helped in finding out what was happening in a single cardiac cycle. The Wiggers diagram embodies all the available graphical modes and is an accurate testament to what happens during a cardiac cycle.
The Wiggers diagram has ruled for more than a hundred years. It has been a major physiological tool in understanding the function of the heart. Investigations to visualise the beating heart by echocardiography, CT scan, and MRI, with further investigative combinations and modifications, occurred in the latter part of this millennium. Interestingly enough, none of these finds a place in modifications of the Wiggers diagram. The events in a single cardiac cycle may be summarised as follows:

1. Passive atrial filling with venous blood. 2. Atrial contraction in the late phase, with the full opening of the atrioventricular valves for driving the blood into the passively filling ventricles. 3. Stretching of myocytes of the ventricles to the limits of Starling’s law. 4. Isovolumetric contraction and the first heart sound due to the closure of the atrioventricular valves. 5. Contraction of the left and right ventricular muscle in unison, or systole, to pump blood into the respective systemic and pulmonary circulations. 6. Completion of the forced ejection, or systole, and the 2nd heart sound prevent backflow of ejected blood into the ventricles. 7. The 2nd heart sound indicates closure of the semilunar or atrioventricular & ventriculo-arterial valves. 8. Isovolumetric relaxation starts. 9. A small reverberative 3rd heart sound may be audible, indicating turbulence of blood in mid diastole. 10. Total diastolic relaxation of the heart before spontaneous initiation of a new cycle.
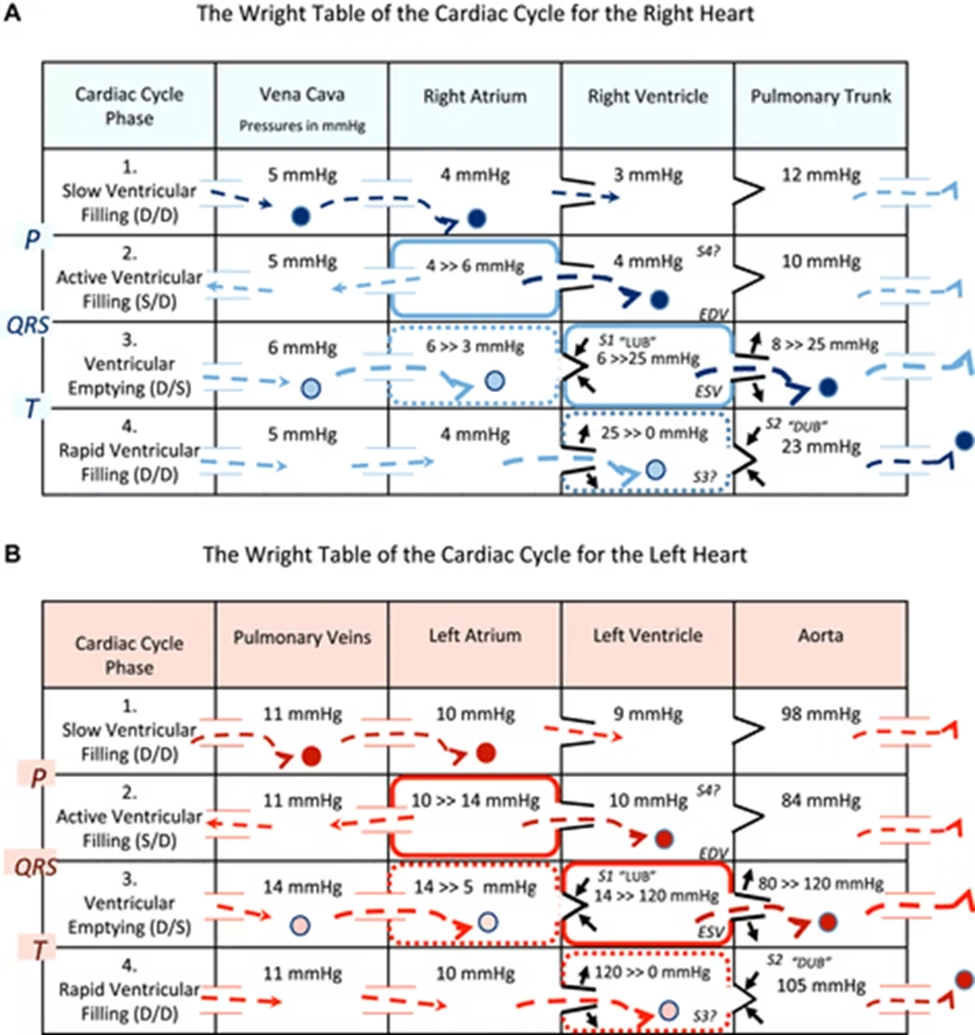
In 2020, a new Wright diagram was proposed separately, indicating left and right ventricular and atrial cavitary pressure changes in conjunction with the events. This is Wright’s table and is as follows:
Aristotle, way back in time, is considered the first person to recognize the heart as the central and most important organ of an individual. However, he could not alienate himself from the mystical ideas that surrounded the organ taught at that time. He was accurate as he was bold enough to state that the heart was “the source of all movement since the heart links the soul with the organs of life. The rhythmical and constant beat of the heart from birth to death was well-known from the very beginning. That the upstroke of the pulse coincides with the contraction of the heart was also well known. Though early Egyptians are credited with this fact, this fact was universal, and some clinical practices even emphasised the importance of the pulse examination. The Ayurvedic practice had ‘vayu’, ‘pitta’, and ‘kaph’ as equivalents of the four humours in Western medicine. The pulse was also known as the ’nari’ with a broader accent to the ‘r’ and the tip of the three fingers was used to examine the pulse. A thorough examination of the pulse and understanding of the physical and mental state of a person, together with the ability to predict the course of the disease, was considered supreme.
The Greeks introduced the term ‘cardia' for the heart and also called the earlike projections, the ‘auricles’, after veins joined the heart. Leonardo da Vinci first recognised that the human heart was four-chambered. The thick-walled ventricles were the actual pumping chambers.
With Harvey’s revolutionary theory of the method of circulation, the horizon opened for the development of techniques for visualization of the beating organ.
In 1896, Rehn created a feat which was considered a landmark. He was made to repair a right
ventricular stab wound with two interrupted horsehair sutures mounted on the smallest and thinnest needle available at that time. This was the beginning of cardiac surgery. Discovery and use of heparin, DeBakey’s promotion of Porter-Bradley pump as the Heart-Lung machine, Gibbon’s successful use of the heart-lung machine for repair of an intracardiac defect, and gradual evolution of the oxygenators were, among other factors, responsible for the improved state of cardiac surgery today.
Proper and accurate diagnosis of a disease is important. Logical progression of thought, objective observation, patient hearing of the presenting complaints and symptoms, acute observation and understanding of the characteristic signs, and interpretation of relevant clinical methods helps in arriving at a provisional diagnosis. There may be more than one provisional diagnosis. This is followed by directed laboratory and imaging investigations to help in making the final diagnosis. Definitive diagnosis should be logical and scientific.


Comments